
With this growing clinical evidence, RetiCap®DR emerges as a science-backed support for the diabetic retina.
(R)-alpha lipoic acid, capsule shell (hydroxypropyl methylcellulose, colorants: iron oxides and hydroxides), bulking agent: microcrystalline cellulose; rutin (rutoside trihydrate), anti-caking agent: silicon dioxide, magnesium salts of fatty acids; Vitamin B2 (riboflavin-5-phosphate sodium), vitamin B1 (thiamine mononitrate).
Nutritional Information | Per Daily Dose (1 capsule) | Reference Intake (per capsule)* |
|---|---|---|
(R)-α-lipoic acid | 150 mg | ** |
Vitamin B2 | 1,1 mg | 100% |
Vitamin B2 | 1,4 mg | 100% |
Rutin | 25 mg | ** |
* Percentage of the reference intake by EU Regulation 1169/2011
** no nutrient reference values available/ no EU recommendation available
Patients should take one capsule daily, approximately 1–2 hours before a meal, with a small amount of liquid, swallowing the capsule whole.
Alpha-lipoic acid (ALA) is best absorbed on an empty stomach. If taken with food — especially with fatty or protein-rich meals — the absorption of ALA is significantly reduced. Studies show that ALA competes with other nutrients for transport and that food can lower the bioavailability.
Before a meal = higher absorption.
With food = reduced effectiveness.
Furthermore, ALA chelates metals. Since metal chelation can influence dietary intake, it is important to take RetiCap®DR with sufficient intervals between meals to avoid interference with the absorption of essential minerals, such as iron and zinc.
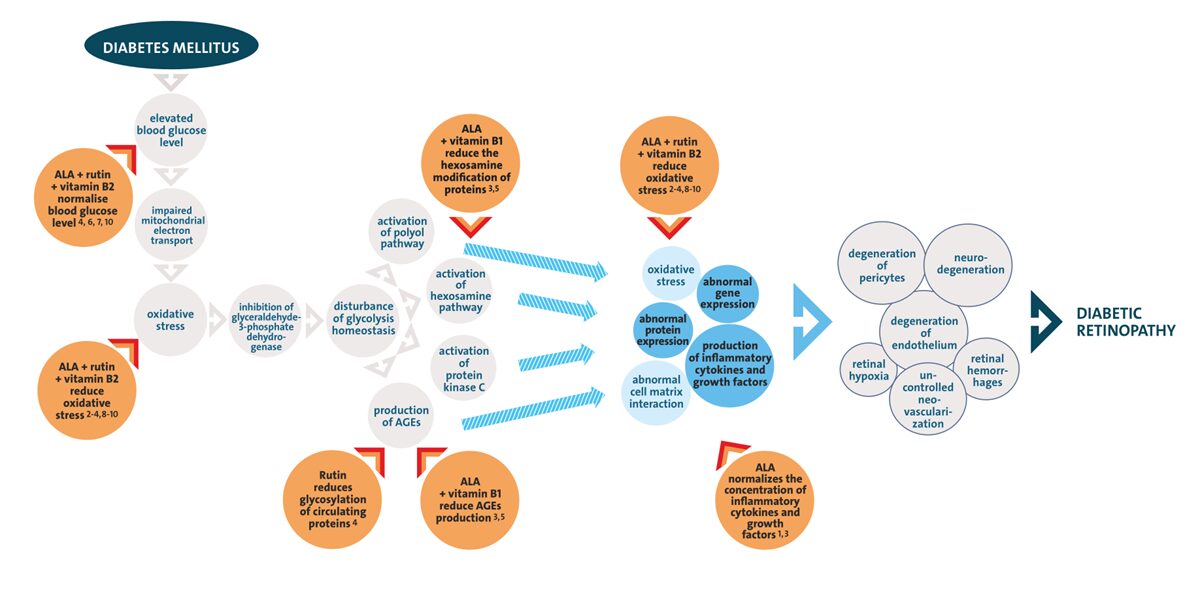
The complex pathogenesis of diabetic retinopathy (DR) is triggered by hyperglycaemia-induced oxidative stress (OS), which damages capillary endothelial cells, nerve cells, and glial cells in the retina. Increased OS leads to changes in cellular metabolism, including:
These mechanisms further amplify oxidative stress, promote the production of pro-inflammatory cytokines and growth factors, and result in vascular abnormalities as well as increased apoptosis. The micronutrient complex in RetiCap®DR is designed to interrupt these pathological processes and support retinal health.
Alpha-lipoic acid (ALA) is a naturally occurring dithiol compound known for its antioxidant and metal-chelating properties. ALA is produced in the body either enzymatically in mitochondria or ingested through food. R-alpha-lipoic acid is the biologically active enantiomer that serves as a cofactor for mitochondrial enzymes.
R-alpha-lipoic acid:
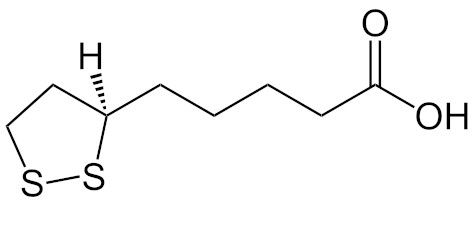
Alpha-lipoic acid (ALA) is a chiral molecule that exists as two enantiomers: (R)-ALA and (S)-ALA. Both forms are reduced within cells to dihydrolipoic acid (DHLA), a potent natural antioxidant. However, only the (R)-enantiomer functions as a cofactor for essential mitochondrial enzyme complexes, such as pyruvate dehydrogenase, making it critical for cellular energy metabolism. Additionally, (R)-ALA demonstrates greater oral bioavailability than (S)-ALA.
Extensive clinical studies (e.g., ALADIN, SYDNEY, ORPIL) have confirmed the safety of high-dose ALA under controlled conditions. Nonetheless, emerging scientific discussions and regulatory reviews are increasingly focusing on theoretical risks, such as mineral chelation effects and rare autoimmune reactions in genetically predisposed individuals.
In anticipation of evolving regulatory expectations and to proactively align with the highest safety standards, we have optimised the RetiCap®DR formulation. By reducing the total ALA content while preserving the full efficacy of the bioactive (R)-ALA form, we ensure the product continues to deliver mitochondrial and antioxidant benefits—while minimizing non-essential exposure.
New formulation: One daily capsule now provides 150 mg of pure (R)-alpha-lipoic acid, whereas the previous formulation contained 300 mg of racemic DL-alpha-lipoic acid—a 50:50 mixture of the biologically active (R)- and the inactive (S)-enantiomer. Since only the (R)-form serves as a cofactor for essential mitochondrial enzyme complexes, the effect on mitochondrial energy metabolism remains unchanged. In addition, the gelatin-based capsule shell has been replaced with a hydroxypropyl methylcellulose (HPMC) shell. HPMC is vegan and therefore makes RetiCap®DR more suitable for certain patients.
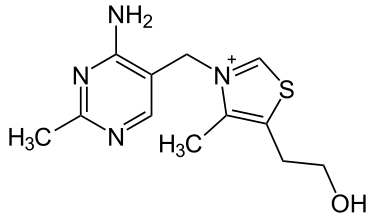
Also known as thiamine, vitamin B1 consists of a pyrimidine ring connected to a thiazole ring via a methyl group. It is ingested with food and then converted into the biologically active form thiamine diphosphate (TPP). As a coenzyme, TPP is involved in the metabolism of carbohydrates, amino acids and fatty acids.
Vitamin B1:
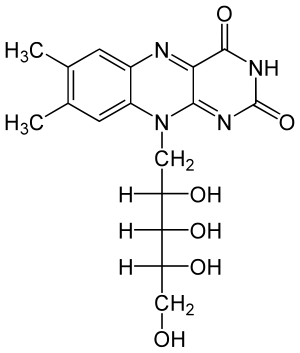
Also known as riboflavin, vitamin B2 is the precursor to the coenzymes flavin adenine dinucleotide (FAD) and flavin mononucleotide (FMN). Both FAD
and FMN function as electron carriers in various redox reactions, playing a key role in numerous metabolic pathways.
Vitamin B2:
Rutin belongs to the group of bioflavonoids and is known for its vascular stabilising, antiinflammatory and antioxidant effects.
Rutin:
Did you know that eye care professionals can request free samples of RetiCap®DR here?
The evaluation of a therapeutic approach requires not only evidence of statistical significance but also an assessment of the clinical relevance of the results.
While statistical significance indicates that an observed effect is highly likely to be reproducible (typically at a 95% confidence level), analysing the effect size provides additional insights into the practical significance of this effect for patient care.
To comprehensively assess the effectiveness of micronutrient supplementation, differences in contrast sensitivity (CS) at various time points were analysed using ANOVA and the Kruskal-Wallis test. Additionally, the effect size of six months of supplementation was calculated using Cohen’s d metric.
The effect size d classifies clinical relevance as follows:
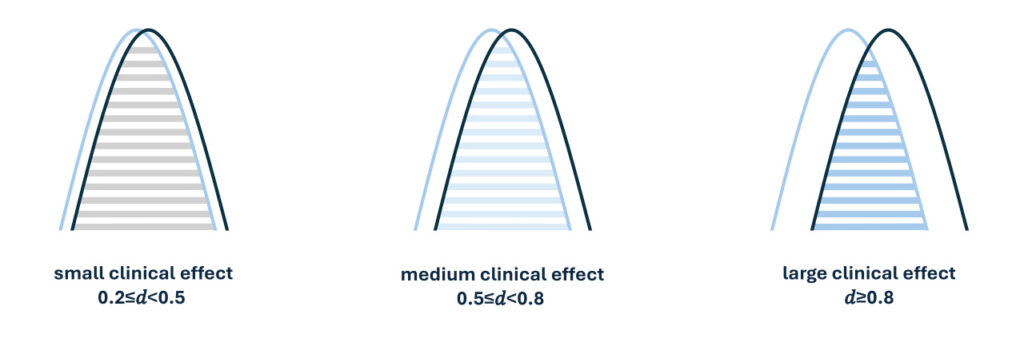
This approach makes it possible to assess the actual impact of supplementation on patients beyond mere statistical significance.
The effect size was calculated for all supplemented groups to assess the clinical relevance of micronutrient supplementation. The results showed:
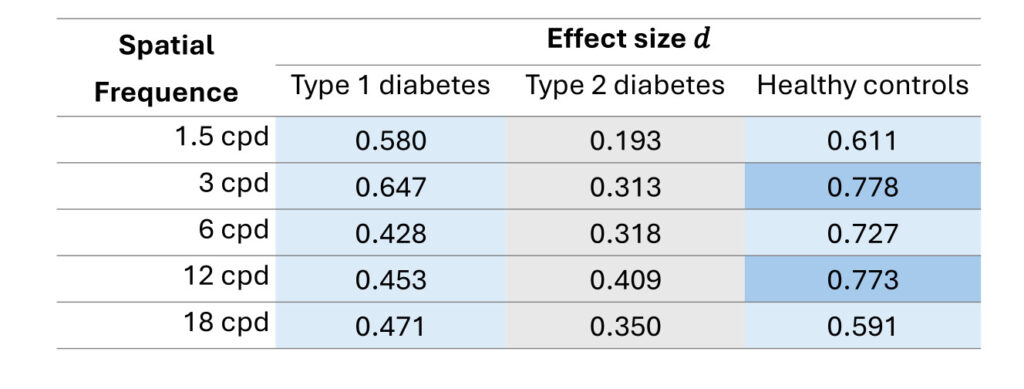
In summary, the analysis shows that micronutrient supplementation with the examined complex not only produces reproducible results but also leads to clinically relevant improvements in patients.
Watch this video with Dr. Franziska Wirth, where she presents exciting study results on the effects of alpha-lipoic acid, vitamins B1 and B2, and rutin on diabetic eyes at this year’s Conference of the German Ophthalmological Society (DOG 2024) in Berlin.
For a closer look at the poster, click here: https://ebiga-vision.com/wp-content/uploads/2024/11/ebiga-VISION_Poster_Micronutrient-Supplementation-in-Diabetic-Patients.pdf
ebiga-VISION aims to give medical professionals the opportunity to assess the product, provide their patients with comprehensive and straightforward advice, and offer them an evidence-based option for the management of diabetic eyes.
Research Team | Year | Duration | Design | Participant Demographics | Results |
|---|---|---|---|---|---|
Wirth et. al. | 2024 | 6 months | Case-control study |
|
|
Mulak et al. | 2019 | 6 months |
Observational study |
|
|
Ciszewska et al. | 2017 | 6 months |
Observational study |
|
|
Gebka et al. | 2014 | 3 months | Case-control study |
|
|
Please contact us using our contact form. We would be happy to send you a PDF with our current prices and discount levels for practice shop owners. You can also easily reach us by phone to place an order.
In most countries, patients can conveniently order RetiCap®DR from selected pharmacies or trusted online retailers. It is also available through the official distributors, ebiga-VISION and VivaQuity, and their authorised partner shops. Simply click on your country flag to be redirected to the relevant shop page.
This content is intended solely for the eyes of healthcare professionals. Please confirm below: